Divya is 33. She’s a software architect in Pune, mother of a 14-month-old, and she’s been picking hair off the bathroom floor in handfuls since her daughter was four months old. Her temple hairline has receded by about two centimetres on each side. The parting has visibly widened. Under bathroom light, she can see scalp through the crown. She’s done all the things you’re supposed to do as an Indian woman with hair fall. TSH came back at 3.8, called normal. Haemoglobin was 12.6, called normal. Vitamin D was 22 ng/mL, called borderline. Two trichology clinics sold her a ₹35,000 PRP package between them. She bought biotin gummies off Instagram and ate them for three months. Took a multivitamin that gave her 10 mg of elemental iron a day. Oiled with bhringraj, then amla, then onion, then a Korean serum a friend got for her.

None of it moved the needle. Her family doctor told her it was “hormonal” and would “settle on its own.”
The reports are not normal. The reports are being read against the wrong scale.
This is the single most useful thing for an Indian woman over 30 to know about her hair fall: most cases aren’t one thing. They’re two. A slow chronic depletion that’s been building for years, plus an acute trigger that finally makes the loss visible. The trigger gets all the attention. The chronic layer is what actually has to be fixed. Most doctors are trained to read for the trigger and miss the substrate underneath it.
What You Are Seeing In The Comb Is Usually The Second Event, Not The First
Female pattern hair loss in India tends to start in the early 30s and shows up in a fairly specific way. The parting widens when you tie your hair. The crown gets thinner under bathroom light. The temples slowly recede. The frontal hairline at the forehead usually holds, which separates it from frontal fibrosing alopecia (a scarring condition that’s a different problem entirely). This is female pattern hair loss (FPHL), the female version of what most Indian men get on top. An Indian dermatology audit pegged male prevalence at 58 percent in the 30-50 band; women’s numbers are underreported but climbing fast.

The Ludwig scale is the standard way to grade it. Stage 1 is mild thinning of the crown. Stage 2 is moderate thinning with visible scalp through the parting in bright light. Stage 3 is severe thinning with extensive scalp visibility. Most Indian women who walk in at 33 are sitting at Ludwig 1 to 2, which is exactly the stage where doing the right thing actually works.
And here’s the part that gets missed. In most women who come in for sudden hair fall after 30, FPHL has been quietly progressing in the background for years, slow enough that nobody clocks it. Then a trigger fires (pregnancy and the postpartum hormone crash, a bout of dengue or typhoid, a crash diet, a COVID infection, surgery under anaesthesia, a death in the family, a thyroid flare, severe vitamin D deficiency) and the trigger shoves a big chunk of hair into the resting (telogen) phase. Two to three months later, that hair sheds in fistfuls. The name for this is telogen effluvium.
A 2024 study of 200 postpartum women in the Journal of Clinical and Aesthetic Dermatology found only 9.5 percent had pure telogen effluvium. 56 percent had telogen effluvium plus an underlying androgenetic alopecia that had been hiding underneath. That’s why the hair “never quite comes back” after the trigger event. The acute shed recovers in six to nine months. The underlying pattern loss does not. Two different problems, one moment of becoming visible.
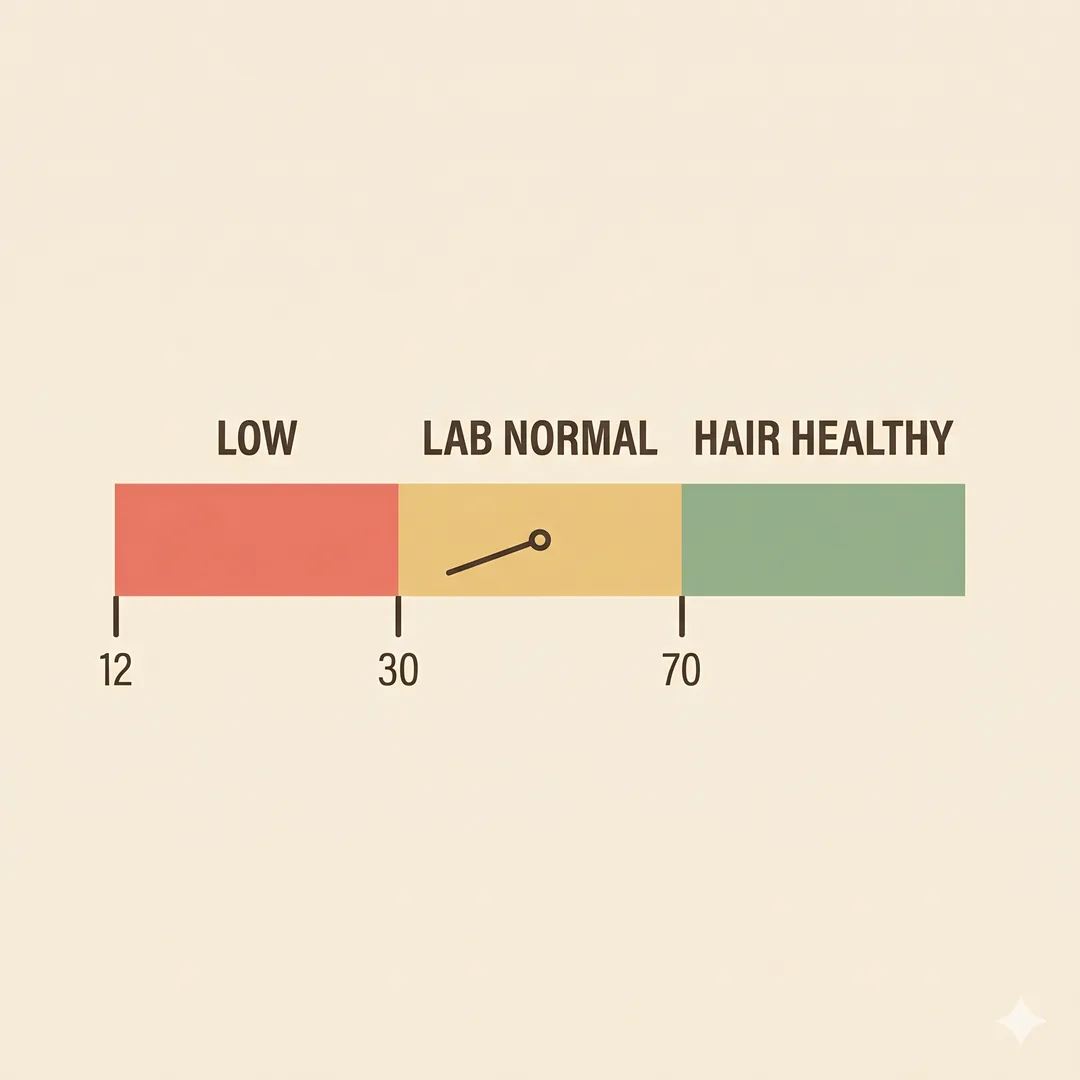
The Ferritin Number Your Lab Calls “Normal” Is Not Normal For Hair
If you’ve ever been handed a lab report that says “Serum Ferritin: 18 ng/mL — Within Normal Range (12-150)” and been told your iron is fine, you’ve been failed by the way reference ranges are written.
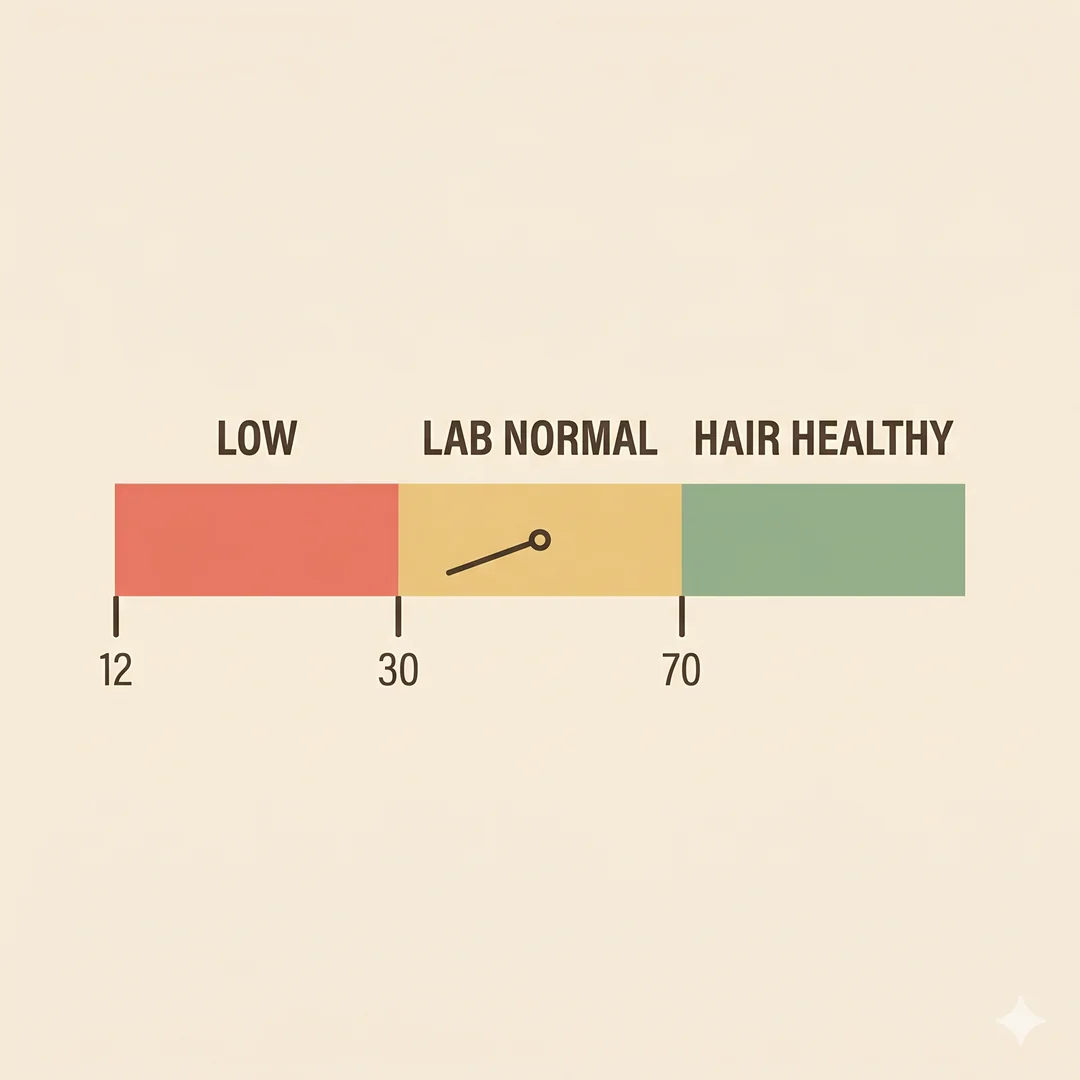
The 12 ng/mL lower limit on Indian lab reports was set to catch frank iron-deficiency anaemia, the kind that makes you breathless climbing stairs. It wasn’t drawn for adequate hair iron stores. Trichology research across the last two decades is consistent on this. Ferritin needs to sit above roughly 70 ng/mL for shedding to stop and for new growth to come in healthily. In one major female alopecia review, 70 percent of women with diffuse shedding had ferritin below 30 ng/mL, sitting well within the “normal” range as most labs print it. The 2007 Trost paper in the Journal of the American Academy of Dermatology told dermatologists to treat ferritin under 40 ng/mL as low, no matter what the lab range said. The 2022 JAMA Dermatology meta-analysis on iron deficiency and nonscarring alopecia in women confirmed the association across multiple studies.
For Indian women in their 30s, this gap matters more than anywhere else on earth. NFHS-5 (2019-21) found that 57 percent of Indian women aged 15-49 are anaemic, up from 53 percent in NFHS-4. The two structural reasons are well known. Predominantly vegetarian iron intake is non-heme iron from dal, palak and ragi, absorbed two to three times less efficiently than heme iron from non-veg, fish or eggs. Monthly menstrual blood loss compounds the deficit, and the average Indian diet doesn’t keep up. A woman who had borderline-low iron at 24 has severely depleted iron at 34 after two pregnancies, two years of breastfeeding, and a decade of average periods.
The fix isn’t a multivitamin capsule with 10 mg of elemental iron. The fix is an actual ferritin test (ask for it explicitly, since most “iron panels” report only haemoglobin and serum iron) and, if the number is under 70 ng/mL, a proper iron correction over three to six months guided by a physician.
The Four Other Layers Underneath
Ferritin is the most common chronic cause. It’s rarely alone. There are four others that turn up in almost every Indian hair-fall workup, and every one of them has to be checked before anyone accepts “everything is normal.”
Vitamin D. An Indian analytical study in the Indian Journal of Dermatopathology and Diagnostic Dermatology found significantly lower vitamin D levels in women with diffuse hair loss compared to controls. Given that 60 to 90 percent of urban Indians are deficient regardless of the hair question, this is almost a guaranteed second hit. Get the 25-OH-D test done at the same time as ferritin. Target a level above 30 ng/mL; many dermatologists prefer 40 to 50 ng/mL for hair specifically.
Thyroid. Both hypothyroidism and hyperthyroidism cause hair shedding. Hypothyroidism is the more common one in Indian women. About 15 percent of adult women have it, often undiagnosed. Even subclinical hypothyroidism with TSH between 5 and 10 mIU/L can present as diffuse hair shedding. Insist on a full TSH plus Free T4 plus anti-TPO panel, not just TSH alone. If TSH is above 2.5 and hair is falling, treatment can be considered even though the number sits in the “normal” range. (And if you are already on Eltroxin and your hair is still falling, the first place to look is whether the medicine is being absorbed properly. The morning chai-and-calcium routine quietly cancels 30 to 40 percent of every dose.)
PCOS. Female pattern hair loss and PCOS are bidirectionally linked. A 2024 systematic review and meta-analysis of 24 observational studies confirmed the association. If you have irregular periods, jaw-line acne, dark patches on the neck (acanthosis nigricans), or weight gain around the middle, your hair fall has an endocrine layer that no amount of hair oil will touch. Get a basic PCOS workup. Testosterone, DHEAS, fasting insulin, ultrasound.
Crash diets, intermittent fasting, and protein shortfalls. The single fastest way to push your hair into a telogen shed is sudden severe calorie restriction. The “16:8 plus only-salad-for-dinner” routine that became popular post-pandemic among urban Indian women is a near-perfect recipe for telogen effluvium three months out. Hair is made of keratin, a protein, and Indian vegetarian diets often run low on complete protein anyway. If you weigh 60 kg, you need roughly 70 to 90 grams of protein a day for hair to maintain itself. That’s two egg whites, one bowl of dal, one bowl of curd, one fistful of paneer or sprouts, and possibly a 20 to 30 g whey protein scoop. Most middle-class Indian women on a “healthy diet” eat half of that. Add a busy postpartum year or a diet phase on top, and the hair shows it three months down the line.
Vitamin B12 and zinc. Often low in Indian vegetarian women, both required for keratin synthesis. B12 below 300 pg/mL and serum zinc below 70 µg/dL should be corrected. Test alongside ferritin.
The Full Diagnostic Workup — Order Of Tests
Get the complete panel in one go, otherwise you’ll lose the typical four-month diagnostic delay to back-and-forth visits in Indian primary care.

Ferritin (true marker of iron stores). Target >70 ng/mL for hair. ₹500 to ₹800.
Complete blood count with peripheral smear, for anaemia type and inflammation.
25-hydroxyvitamin D, target >40 ng/mL.
TSH, Free T4, anti-TPO antibodies, for thyroid function and autoimmunity.
Total testosterone, DHEAS, SHBG, fasting insulin, HbA1c, if PCOS is suspected.
Vitamin B12 and folate, vegetarian women especially.
Serum zinc, if symptoms include white spots on nails or skin changes.
ANA, ESR, CRP, if hair fall is patchy, has skin lesions, or comes with joint pain (rule out lupus, alopecia areata).
Pull test, done by a dermatologist in clinic. Gentle traction of 50 hairs from three scalp areas. More than 6 hairs coming out means active shedding.
Trichoscopy, dermatoscopy of the scalp. Differentiates FPHL from telogen effluvium and detects miniaturisation.
Total Indian cost for the comprehensive panel: ₹2,500 to ₹4,500 at major diagnostic chains.
Treatment Ladder — The Order Matters
Step 1 — Correct the substrate. Wherever the numbers are low, fix them with a physician-supervised plan. Oral iron 60 to 100 mg elemental iron daily (ferrous fumarate, ferrous sulfate or ferrous ascorbate) taken with vitamin C (a glass of orange juice or amla water) on an empty stomach. Critically, not with chai or coffee, which block iron absorption the same way they block thyroxine. Alternate-day dosing actually absorbs iron better than daily on current evidence. Stoffel’s 2017 Lancet Haematology paper showed 2x absorption with fewer GI side effects. Take iron at lunch with a glass of nimbu pani if morning timing doesn’t work. IV ferric carboxymaltose 1000 mg single dose is now widely available in India at ₹4500 to ₹7000 and is appropriate for severe deficiency or those who can’t tolerate oral iron. It corrects stores in weeks rather than months. Vitamin D loading and maintenance per the Indian Endocrine Society 2025 consensus. Thyroid and PCOS management as indicated.

Step 2 — Protein and basics. Hit 1.2 to 1.6 g protein per kg body weight daily. Add a 20 g whey protein scoop after exercise. Two eggs daily for non-vegetarians. Two egg whites plus a dal-paneer-curd combination for ovo-vegetarians. Doubled dal-paneer-sprouts-soya combinations for pure-vegetarians. Adequate calories matter too; under-eating shuts hair down regardless of nutrient adequacy.
Step 3 — Mechanical. Stop tight ponytails and tight braids that cause traction alopecia at the temples, a major contributor for Indian women who tie their hair tight for work or kitchen reasons every single day. Switch to satin pillowcases. Avoid heavy daily oil massages with vigorous rubbing on hair that’s already shedding; gentle scalp oiling once or twice a week is enough. Heat tools, harsh chemical treatments, daily tight buns. All minor contributors that add up.
Step 4 — Topical minoxidil. Only after three months of substrate correction. Topical 2% or 5% minoxidil applied to a clean dry scalp once or twice daily is the most evidence-backed intervention for female pattern loss. Visible improvement typically takes six to twelve months. The 5% solution shows superior efficacy in trials but with a slightly higher risk of facial hypertrichosis, which often resolves on dose reduction. Stopping minoxidil means losing the regrowth gradually. Cost in India: ₹400 to ₹800 per month.
Step 5 — Oral spironolactone or low-dose oral minoxidil. For non-responders or progressive cases, dermatology-supervised second-line options. A 2023 PMC10502763 systematic review and meta-analysis confirmed oral spironolactone 50 to 200 mg daily is effective for female pattern hair loss in women. A 2024 RCT in Journal of Cosmetic Dermatology showed combination topical minoxidil 2% plus oral spironolactone 100 mg daily produced 50 percent good responder rates at 4 months. Low-dose oral minoxidil 0.25 to 1 mg daily has also emerged as effective in real-world studies, with the advantage of better compliance than topical. Both require monitoring for side effects (spironolactone: hyperkalaemia, irregular periods; oral minoxidil: hypertrichosis, pedal oedema).
Step 6 — Procedures (only after substrate is fixed). Platelet-rich plasma (PRP) injections monthly for 4 to 6 sessions, then maintenance every 4 to 6 months. A 2024 systematic review and meta-analysis (PMC11342464) confirmed significant hair density improvements in female pattern hair loss. Cost: ₹4000 to ₹8000 per session in India. Low-level laser therapy (LLLT) caps and combs have moderate evidence; a 2024 review showed effectiveness in mild-to-moderate FPHL. Microneedling combined with minoxidil produces additive results. Hair transplantation for non-responders with stable donor density.
Step 7 — Maintenance. Hair takes a year to tell you whether something is working. Most Indian women abandon a protocol at the four-month mark because “nothing is happening.” Four months in is exactly when the first new anagen hairs are starting to push through. Stay the course. Annual ferritin and Vitamin D rechecks to prevent relapse.
When To Actually See A Dermatologist Urgently
If you’re losing more than 100 strands a day for over three months, if you can see scalp through your parting in normal indoor light, if the temples are visibly receding, if hair fall is paired with sudden weight changes, irregular periods, or visible thinning of eyebrows, book a dermatologist, not a hair clinic. Hair clinics sell packages. Dermatologists order the right tests and prescribe what is actually needed.
Same-week dermatology evaluation is warranted for: patchy hair loss with bald spots (alopecia areata, may need intralesional steroids); scarring areas with no follicular openings (frontal fibrosing alopecia, lichen planopilaris, irreversible if missed); hair fall with skin rash on face or arms (rule out lupus); sudden severe shedding with rapid scalp visibility (rule out telogen effluvium from a serious systemic illness); hair fall in pregnancy with severe nausea, fatigue, or palpitations (rule out hyperthyroidism, severe anaemia).
What Indian Women Who Got Their Hair Back Actually Did
The patterns from Indian women’s health groups and r/Indian_Hair are consistent.

“Fixed my ferritin from 22 to 78 over six months using IV ferric carboxymaltose plus diet. Hair fall stopped at month four. New growth at month eight.”
“Got my vitamin D from 14 to 48 with proper sachet schedule plus magnesium plus full-fat milk with the dose. Hair stopped falling around month three of normalised levels.”
“Spironolactone 50 mg plus topical minoxidil 5%. Lifesaver after three years of PRP that didn’t really do much.”
“Stopped the intermittent fasting. Started eating two boiled eggs plus a whey scoop daily. Hair fall halved in eight weeks.”
“Discovered I had subclinical hypothyroidism with TSH of 5.8 that everyone said was ‘normal.’ Doctor started Eltroxin 25 mcg. Hair fall reduced significantly in three months.”
“PRP did nothing on its own. PRP combined with corrected ferritin, vitamin D, and minoxidil was the combination that worked.”
The pattern is the same every time. Substrate first, then medical treatment, then procedures. Going in the reverse order, procedures first, is what most Indian women try and what eats through ₹50,000 to ₹2 lakh before anyone gets honest about it.

Also Read
Blood Sugar Balance at Social Events — a Diabetic’s Discreet Guide
For pharma distributors and clinicians looking for quality-assured iron formulations (ferrous fumarate, ferrous ascorbate, IV preparations), Vitamin D3 60K and daily-dose tablets, biotin, zinc, B-complex, topical minoxidil 2% and 5%, oral spironolactone, and other dermatology-support formulations, see the IndiaPharmaFranchise product portfolio. Medical professionals exploring distribution partnerships are welcome to get in touch.
Disclaimer
This article is for general health education and isn’t a substitute for personal medical advice. Get your blood work done and consult a qualified dermatologist or physician before starting any iron, vitamin D, minoxidil, spironolactone or hormonal treatment for hair loss. Dose decisions must be made on an individual basis.
Sources
- Prevalence, severity and associated factor of androgenetic alopecia in the dermatology outpatient clinic. IP Indian J Clin Exp Dermatol Vol 5, Issue 4. https://www.ijced.org/
- Postpartum Telogen Effluvium Unmasking Additional Latent Hair Loss Disorders. J Clin Aesthet Dermatol 2024;17(5):15-20.
- Trost LB, Bergfeld WF, Calogeras E. The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. J Am Acad Dermatol 2006;54(5):824-44.
- Iron Deficiency and Nonscarring Alopecia in Women: Systematic Review and Meta-Analysis. JAMA Dermatol 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC8928181/
- NFHS-5 India report 2019-2021 — anaemia prevalence in Indian women. https://rchiips.org/nfhs/
- Rammohan A et al. Plant-Based Dietary Practices and Socioeconomic Factors That Influence Anemia in India. Nutrients 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8537570/
- An Analytical Study of Serum Ferritin, Vitamin D, and Thyroid Function in Females with Diffuse Hair Loss. Indian J Dermatopathol Diagn Dermatol 2022;9(1).
- Bi-directional association between female pattern hair loss and polycystic ovary syndrome: A systematic review and meta-analysis. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC12481967/
- The Efficacy and Safety of Oral Spironolactone in the Treatment of Female Pattern Hair Loss: A Systematic Review and Meta-Analysis. PMC 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10502763/
- Sadeghzadeh Bazargan A et al. The efficacy of the combination of topical minoxidil and oral spironolactone compared with the combination of topical minoxidil and oral finasteride in women with androgenic alopecia. Journal of Cosmetic Dermatology 2024. https://onlinelibrary.wiley.com/doi/10.1111/jocd.15979
- Effectiveness of platelet-rich plasma in treating female hair loss: A systematic review and meta-analysis of randomized controlled trials. PMC 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11342464/
- Gentile P, Garcovich S. The Effectiveness of Low-Level Light/Laser Therapy on Hair Loss. 2024. https://journals.sagepub.com/doi/10.1089/jocd.15979
- Effectiveness of platelet-rich plasma in treating female hair loss: A systematic review and meta-analysis of randomized controlled trials. PMC 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11342464/
- Gentile P, Garcovich S. The Effectiveness of Low-Level Light/Laser Therapy on Hair Loss. 2024. https://journals.sagepub.com/doi/10.1089/fpsam.2021.0151
- Stoffel NU et al. Iron absorption from oral iron supplements given on consecutive versus alternate days. Lancet Haematology 2017.
You might also like

How Does Monobenzone Work? Mechanism of Action Explained
How Does Monobenzone Work? Mechanism of Action Explained Monobenzone is prescription-only. This article explains the cellular mechanism so…
Read article →
Michael Jackson & Monobenzone — Separating Medical Fact from Myth
Michael Jackson & Monobenzone — Separating Medical Fact from Myth A note on this article. Discussions of Michael…
Read article →
Belly Fat Won’t Budge in India Even Though You’re Eating Less? It’s Probably Not About Calories
South Asians carry roughly twice the visceral fat at the same BMI — which is why generic "eat…
Read article →