
Anjali is 38. HR head at a mid-sized Gurgaon firm. She’s been “watching her weight” for about a decade now, the way most women her age have.
Her body mass index (BMI) sits at 22.8, which is clinically normal. She walks 7,000 steps a day. She quit the late-night Maggi habit, moved to brown bread, swapped basmati for handpounded rice, gave up the second roti at lunch. Six months later, the scale has shifted down by 1.4 kg. The belly, though, is exactly where it was three years ago. Her tailor recently asked, with that particular kind of gentleness that lands harder than a slap, whether she’d like the waist a little looser this time around.
If you’re reading this and quietly nodding, you’re not alone. Not even close.
This pattern is so common in India that metabolic medicine has a quiet name for it. South Asians are some of the most under-served readers of the generic “eat less, move more” advice that fills English-language diet content. The thing we struggle with most — visceral abdominal fat, the kind that wraps around the organs — barely responds to the strategy most diet articles push. Once you see what’s going on underneath, the fix becomes weirdly specific. Let’s walk through it.
The thin-fat Indian — why your belly doesn’t match your BMI

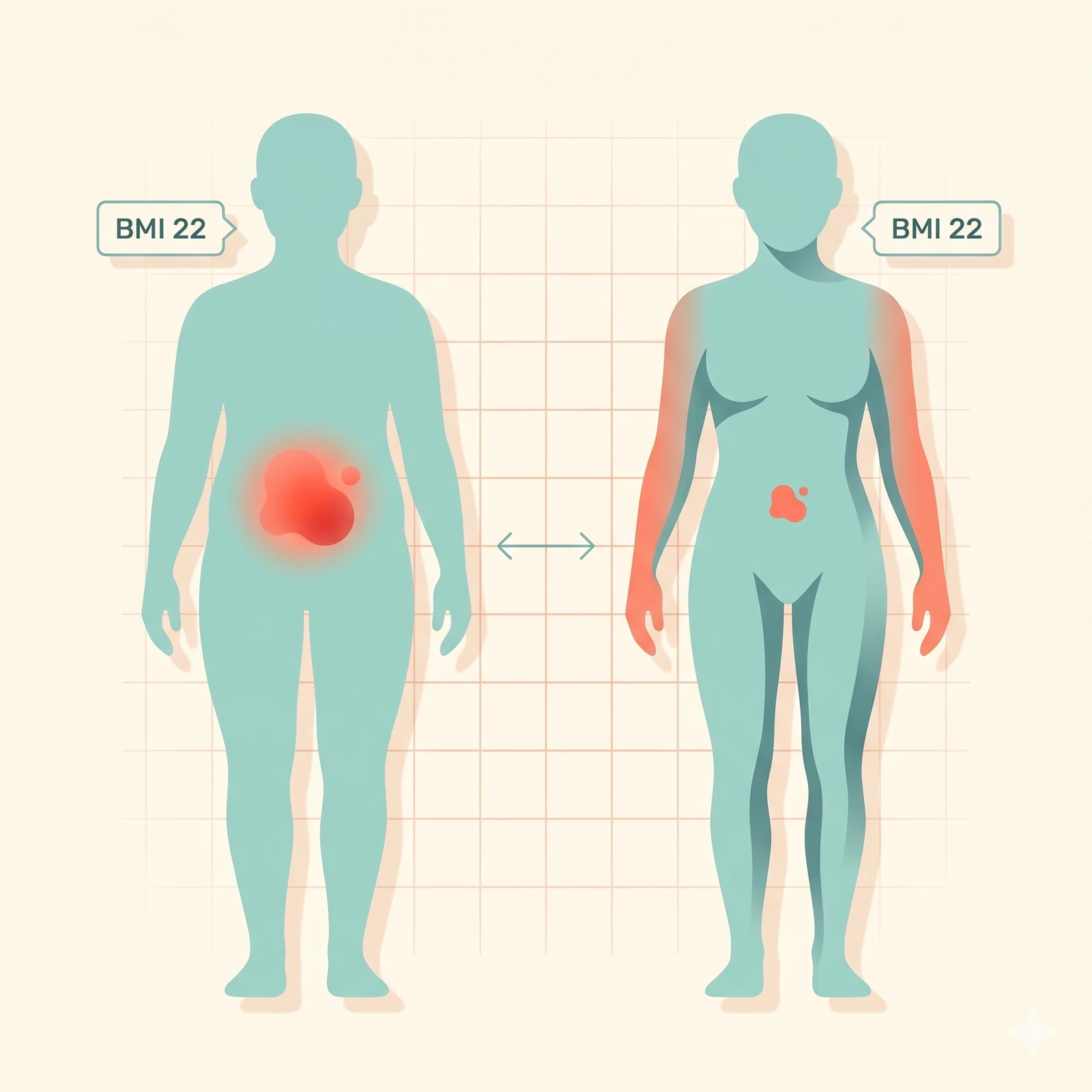
The literature on this is now overwhelming. South Asians display what’s called the Asian Indian phenotype, sometimes called the “thin-fat” phenotype. At the same body weight and BMI as someone of European descent, Indians carry roughly twice the visceral fat (the deep, organ-wrapping kind) and notably less subcutaneous fat on the limbs and hips.
The 2024 Nature Metabolism GlasVEGAS study (article s42255-024-01101-z) put South Asian and white European men side by side, gaining the same amount of weight under controlled conditions. The South Asian men gained less lean tissue. They deposited more of the gained mass as visceral and hepatic fat. They developed insulin resistance at a sharply lower threshold of weight gain.
A person with a BMI of 22 in Mumbai can carry the visceral fat load of a person with a BMI of 27 in London. Total body weight looks healthy on a chart. The waist tells a different story.
Visceral fat matters in a way subcutaneous fat doesn’t. It dumps free fatty acids straight into the portal vein flowing to the liver, driving hepatic insulin resistance. It secretes inflammatory cytokines like IL-6, TNF-alpha and resistin that travel through the body and quietly stoke low-grade chronic inflammation. The 2024 Lancet Diabetes & Endocrinology DXA-based study from Singapore (PubMed 39217997) confirmed that Asian populations show metabolically adverse adiposity at body mass indices that look entirely normal on the usual charts.
So the Indian woman of 58 kg whose belly fat won’t move on a calorie deficit doesn’t have a body-weight problem. She has a body-composition problem. They’re not the same thing.
The Indian numbers are worse than people realise
The ICMR-INDIAB-23 study, published in 2023 in the Indian Journal of Medical Research, surveyed 1,13,043 Indians across 31 states. It found generalised obesity (BMI ≥25) at 28.6 percent and abdominal obesity (waist ≥90 cm in men, ≥80 cm in women) at 39.5 percent. That’s roughly 351 million Indian adults walking around with abdominal obesity by the South Asian-specific cutoffs.
The waist-circumference cutoff matters enormously. International cutoffs of 102 cm for men and 88 cm for women, designed for white European populations, miss most Indian visceral obesity entirely. The correct cutoffs for South Asians are 90 cm and 80 cm respectively. If your tailor is whispering, your tape measure is almost certainly above these.
A 2023 Lancet Regional Health Southeast Asia analysis of NFHS-5 data (PMC10363491) showed that abdominal obesity is now more common in urban Indian women than men. The prevalence has shot up sharply in the last decade across all income groups.
The calorie-deficit trap

Here’s the cruel twist most diet articles won’t tell you. When you cut calories aggressively, especially below 1,200 a day (which most Indian women trying to lose weight end up doing), your body responds in three predictable ways that make belly fat worse, not better.
Cortisol rises. Under-eating is a physiological stressor. Your body releases more cortisol to keep blood sugar up through gluconeogenesis. Cortisol preferentially parks fat at the abdomen via 11-beta-HSD1 enzymes that are densely expressed in visceral fat. The 2012 PMC review on cortisol and metabolic syndrome in South Asians (PMC3405820) documented elevated cortisol responses in this population specifically.
Sleep fragments. Aggressive deficits drop tryptophan and serotonin, which the body needs to make melatonin. Sleep gets shallow and short. Short sleep itself raises cortisol and the hunger hormone ghrelin while dropping leptin. The body then hangs on to visceral fat as an evolved famine response. Logic the calorie spreadsheet doesn’t see.
Muscle goes before fat. Without enough protein and resistance training, weight loss on a deficit comes 30 to 40 percent from lean muscle. Losing muscle drops basal metabolic rate by roughly 20 to 30 kcal per kilogram of muscle, which makes future weight loss harder. The belly, meanwhile, stays put. This is why so many Indians complain that the more they diet, the more they plateau, and the belly never really changes. Only the arms get thinner and the face starts to look tired.
The Indian insulin-resistance problem
The other half of the equation is what we’re actually eating, even on a “diet.” Indians develop insulin resistance at lower BMIs than most other populations. A 2024 PMC paper on cutaneous signs of insulin resistance in South Asians (PMC12708322) noted that acanthosis nigricans, that velvety dark patch on the neck, shows up in over half of South Asian women with central obesity, often before any blood test catches the dysfunction.
The food that drives insulin resistance most aggressively is rapid-release carbohydrate, and the average urban Indian diet is built on it. White rice or polished basmati at lunch and dinner. Refined wheat atta in most household rotis. Two cups of milk-and-sugar chai a day, biscuits on the side. The 4 PM samosa, kachori or vada-pav. Sweets at every wedding, festival, birthday and arrival of relatives. Packaged “healthy” breakfast cereals that are mostly refined carb. Fruit juice and Bournvita sold as nutrition.
You can be in a calorie deficit and still flood your bloodstream with insulin-spiking food every ninety minutes. Insulin is the master fat-storage hormone. When it’s chronically elevated, fat (especially visceral fat) doesn’t get released for burning, no matter what the calorie arithmetic says.
This is the piece that’s missing from most diet conversations. Visceral fat in Indians responds to the type and frequency of carbohydrate more than to total calories. A 1,500 kcal day of three-roti meals plus chai-biscuit twice over will move belly fat less than an 1,800 kcal day of egg-and-paneer breakfast, dal-sabzi-salad lunch, sprouted moong snack, fish-vegetable dinner. Even though the second is higher in calories.
The cortisol-sleep loop you’re probably in

Take honest stock of your last week. How many nights did you sleep under seven hours? How many of those nights did you scroll past midnight? How often did you skip meals and then overeat at 9 PM? How many caffeinated drinks after 4 PM? Did you actually exercise in the morning, or did you sit for ten hours and then watch reels in bed?
Most working-age urban Indians live in a state of chronic mild cortisol elevation. Add the real stressors (Bangalore or Mumbai traffic, EMIs, joint-family politics, ageing parents, work pressure, the WhatsApp group that never sleeps) and cortisol stays up. Cortisol’s pet project, as it happens, is depositing fat around the abdomen.
A 2019 Nutrients paper (PMC6835938) confirmed that fat intake and stress modify the relationship between sleep duration and abdominal obesity. Even people doing everything else right see belly fat sit there when sleep and stress are unmanaged.
You can’t out-diet a broken sleep cycle. You can’t out-walk chronic cortisol. The belly is responsive to these in a way the rest of your body simply isn’t.
Diagnostic workup before you commit to a bigger plan
If you’ve honestly tried for 12 weeks and the belly won’t move, ask your physician for these tests before assuming you’re lazy or eating wrong. Cost in India runs ₹2000 to ₹4000 for the full panel.
Fasting insulin and HOMA-IR (homeostatic model assessment of insulin resistance), not just fasting glucose. HOMA-IR above 2.5 indicates insulin resistance even with normal sugar.
HbA1c and an oral glucose tolerance test. A normal HbA1c of 5.4 alongside a fasting insulin of 22 is actually more dangerous than a slightly elevated HbA1c with a normal insulin.
Thyroid panel: TSH, T3, T4, anti-TPO antibodies. Hypothyroidism is the second most common belly-fat driver in Indian women after PCOS (polycystic ovary syndrome).
PCOS workup for women: testosterone, DHEAS, LH:FSH ratio, pelvic ultrasound. PCOS prevalence in Indian women of reproductive age is 9 to 36 percent, depending on diagnostic criteria.
Liver function and ultrasound abdomen. Non-alcoholic fatty liver disease (now renamed MASLD, metabolic dysfunction-associated steatotic liver disease) is present in roughly 38 percent of Indian adults. It is both cause and consequence of visceral adiposity.
Cortisol if there are clinical signs. 24-hour urinary cortisol or late-night salivary cortisol if you have moon face, easy bruising, purple stretch marks, or proximal muscle weakness. Red flags for Cushing’s syndrome, rare but missable.
Vitamin D. Subnormal in 70 to 90 percent of urban Indians and an independent driver of insulin resistance.
Treatment ladder — in the order it actually works
Step 1 — Protein, properly. Most Indian adults eat 30 to 40 g of protein a day. ICMR’s recommended dietary allowance (RDA) is 0.83 g/kg, but for fat loss with muscle preservation, the body needs 1.2 to 1.6 g per kg body weight. For a 65 kg adult, that’s 80 to 100 g daily. Build every meal around a real protein source. Paneer, eggs, fish, chicken, sprouted moong, soya chunks, hung curd, Greek yoghurt. A 30 g whey protein scoop after exercise is the easiest gap-closer for vegetarians. Plant protein has lower bioavailability, which is why pure vegetarians need 10 to 20 percent more total protein than non-vegetarians for the same outcome.
Step 2 — Resistance training, twice a week, non-negotiable. Indian women are systematically undersold on this. Resistance training — even bodyweight squats, push-ups, planks, and a resistance band at home — preserves muscle, raises basal metabolic rate, improves insulin sensitivity, and shifts body composition in ways aerobic exercise alone can’t. The belly responds to this. Two 30-minute sessions a week is the floor, not the ceiling. Three 45-minute sessions with progressive overload (gradually increasing weights or reps) produce visible waist changes in 12 to 16 weeks even without much scale movement.
Step 3 — Walking after every meal. A 15 to 20 minute walk after lunch and dinner blunts the post-meal glucose spike by 17 to 30 percent in published studies. Three short walks a day beat one long walk for visceral fat. The grandparents knew.
Step 4 — Fix the chai-and-biscuit habit. Swap your two daily sugared chais and biscuits for unsweetened green tea, black coffee, or one chai without sugar plus a boiled egg. That single substitution saves roughly 300 kcal and three big insulin spikes a day without any conscious “dieting.”
Step 5 — Protect seven hours of sleep with a hard phone curfew at 10:30 PM. Sleep restriction below seven hours raises ghrelin, drops leptin, raises evening cortisol and impairs glucose tolerance the next morning. The belly responds to sleep almost as much as it does to food.
Step 6 — Supplements with actual evidence (modest effect sizes). Fenugreek (methi) seed powder, 5 to 10 g daily, has multiple Indian randomised trials behind it for fasting glucose and insulin sensitivity. Cinnamon at 1 to 3 g daily gives a small but real improvement in glucose response. Berberine 500 mg, 2 to 3 times daily, has been compared to metformin in mild insulin resistance with comparable results in some trials. Worth a caution if you’re also on glucose-lowering medication. Magnesium glycinate 200 to 400 mg supports insulin signalling and sleep. Whey protein at 30 g post-exercise is the most reliable way to hit a 1.5 g/kg target on an Indian vegetarian diet.
Step 7 — Medication if BMI and risk justify it. For BMI above 27 with metabolic complications, or above 30 outright, current Indian endocrinology practice now includes consideration of GLP-1 (glucagon-like peptide-1) receptor agonists. Semaglutide (Wegovy, Rybelsus) at appropriate doses produces 12 to 16 percent body weight loss with significant visceral fat reduction. Tirzepatide (Mounjaro) does even better at 18 to 22 percent. Generic semaglutide launched in India in April 2026 at ₹5,660 per month, which is dramatically more accessible than the ₹14,000 to ₹20,000 of branded options. These are real medicines with real side effects: nausea, slowed gastric emptying, pancreatitis risk, gallstones. They should be prescribed by a qualified endocrinologist, not bought from grey-market sellers online. Bariatric surgery (sleeve gastrectomy, gastric bypass) is appropriate for BMI above 35 with complications, or above 40 outright. Cost in India runs ₹3 to 6 lakh.
What Indians who cracked it actually did
Scan Indian PCOS forums, r/india weight-loss threads and Quora India, and the patterns are striking. They’re also consistent.
“Stopped the 4 PM biscuits. Added one boiled egg as a snack. Belly started moving in week 3.”
“Walked after every meal for 15 minutes. Cut chai sugar. Two inches off the waist in 8 weeks. Scale barely moved.”
“Started lifting weights twice a week at age 38. First time the belly actually shrank. Diet alone never did it in fifteen years.”
“Stopped eating after 7:30 PM. Slept by 10:30 PM. Phone curfew at 10. Down 4 kg, mostly from the waist, in three months.”
“Got tested. Found out I had PCOS and undiagnosed insulin resistance. Started metformin plus the protein-and-walking routine. The belly finally responded after six years of trying.”
“Whey protein and Indian vegetarian thali combination. Belly fat moved properly for the first time.”
The solutions are unsexy, repeatable and structural. They are not ten-day detoxes or apple cider vinegar in the morning.
When to stop self-managing and see a doctor
If you have 12 weeks of disciplined effort and the waist hasn’t budged, do the labs. If any of these warning signs show up, see a doctor sooner.
Stubborn belly fat with severe fatigue, hair fall, cold intolerance, constipation — think thyroid. Belly fat with irregular periods, hirsutism, acne — think PCOS. Belly fat with daytime sleepiness, snoring, morning headache — think obstructive sleep apnoea (OSA). Belly fat with moon face, easy bruising, purple stretch marks — think Cushing’s. Belly fat with elevated liver enzymes — think MASLD. Belly fat with HbA1c above 5.7 — think prediabetes. You’re in a five-year window where intervention can stop you sliding into full diabetes.
Don’t assume the belly is cosmetic. Visceral adiposity is the strongest single predictor of cardiometabolic disease in South Asians and an independent risk factor for type 2 diabetes, coronary artery disease, stroke and several cancers including colorectal and breast.
Anjali, by the way, finally got the labs done a few months ago. HOMA-IR was 3.1. Vitamin D was 14. Hypothyroidism, mild. Six months of protein, twice-weekly weights, walks after dinner, a 10:30 PM phone curfew — and the tailor finally said the waist could stay where it was last time. Slow, structural, boring. It worked.

Also Read
How to Reduce Triglycerides Without Medicine in One Month — the same metabolic problem, expressed in a different blood marker.
Blood Sugar Balance at Social Events — A Discreet Diabetic’s Guide — for the eat-out side of the same metabolic story.
For methi seed extract, cinnamon, berberine, magnesium glycinate, and clinical-grade whey protein options, see the full IndiaPharmaFranchise product portfolio. Pharma entrepreneurs interested in bringing high-quality metabolic and weight-management formulations into a regional market can explore the PCD pharma franchise opportunity.
Disclaimer: This article is for general health information only. Stubborn central adiposity can have medical causes that require evaluation. Do not self-prescribe insulin-modifying supplements or GLP-1 medications without proper clinical assessment.
Sources
- GlasVEGAS: Weight gain leads to greater adverse metabolic responses in South Asian compared with white European men. Nature Metabolism 2024. https://www.nature.com/articles/s42255-024-01101-z
- High prevalence of metabolic obesity in India: The ICMR-INDIAB national study (ICMR-INDIAB-23). Indian Journal of Medical Research 2023. https://ijmr.org.in/high-prevalence-of-metabolic-obesity-in-india-the-icmr-indiab-national-study-icmr-indiab-23/
- Abdominal obesity in India: analysis of the National Family Health Survey-5 (2019–2021) data. The Lancet Regional Health Southeast Asia 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10363491/
- Adiposity and metabolic health in Asian populations: an epidemiological study using DXA in Singapore. The Lancet Diabetes & Endocrinology 2024. https://pubmed.ncbi.nlm.nih.gov/39217997/
- Cortisol and the metabolic syndrome in South Asians. PMC 2012. https://pmc.ncbi.nlm.nih.gov/articles/PMC3405820/
- Fat Intake and Stress Modify Sleep Duration Effects on Abdominal Obesity. Nutrients 2019. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6835938/
- Cutaneous signs of insulin resistance with central obesity: insights into adipocentric metabolic dysfunction in South Asians. PMC 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12708322/
- ICMR Dietary Guidelines for Indians — Protein intake recommendations. https://www.nin.res.in/
- Wilding JPH et al. Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine 2021 (STEP-1 trial).
- Jastreboff AM et al. Tirzepatide once weekly for the treatment of obesity. New England Journal of Medicine 2022 (SURMOUNT-1 trial).
You might also like
Monobenzone Before & After — Realistic Timeline Month 1 to Month 12
Monobenzone Before & After — Realistic Timeline Month 1 to Month 12 No real before/after patient photographs are…
Read article →
Monobenzone vs Hydroquinone — Why They Are Not the Same
Monobenzone vs Hydroquinone — Why They Are Not the Same The two compounds are chemically related and often…
Read article →
Monobenzone Side Effects — What’s Expected, What’s a Red Flag
Monobenzone Side Effects — What’s Expected, What’s a Red Flag Monobenzone is prescription-only. This page describes documented side…
Read article →