
Priya is 32, works in product at a Bangalore SaaS company, and eats what her family doctor would call a “perfectly healthy” Indian vegetarian diet. Dal, rice, sabzi, curd at lunch. Roti and a lighter dal at night. The bloating started two years ago: a tight, drum-like feeling that hit around an hour after lunch and stayed until evening tea. She tried cutting wheat. No change. Tried cutting curd. No change. Bought a probiotic from the chemist for ₹890, took it for three weeks, didn’t feel different. Her gastroenterologist did an endoscopy, a celiac panel and a lactose breath test. All normal. He told her to “eat slowly and drink warm water,” wrote out a prescription for a domperidone-PPI combination she didn’t want to take, and that was the end of the visit.
Priya’s case is the most common gut complaint in urban India, and it gets handled badly almost every time. The standard story (weak digestion, take some enzymes) completely misses what’s actually happening in her colon. So let’s get into it properly, because once you understand the mechanism, the fix is mostly free and lives in your own kitchen.
What’s Actually Happening — The GOS Problem
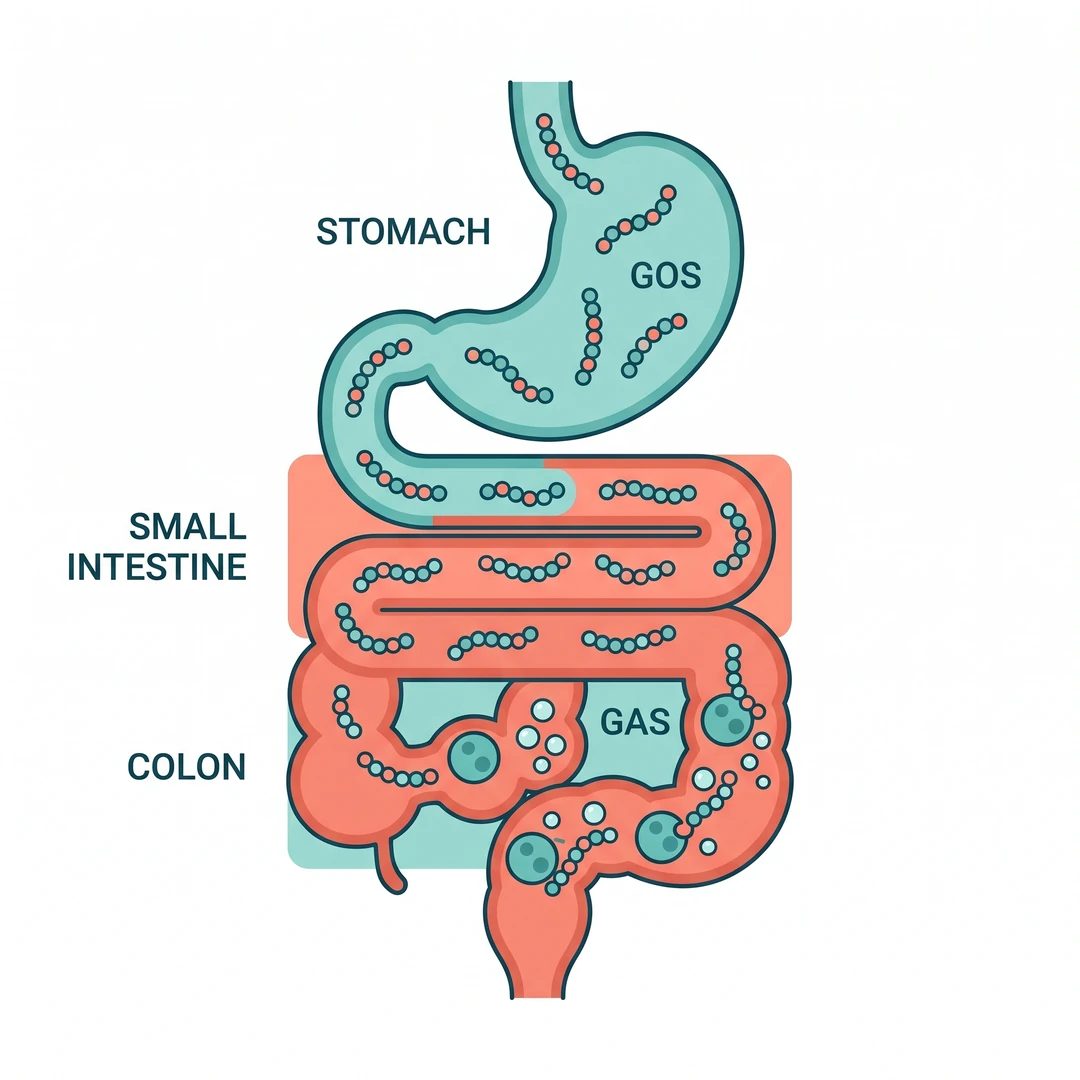
Dal, rajma, chana, chickpeas, kidney beans and to a lesser extent moong all contain a family of carbohydrates called galacto-oligosaccharides (GOS). They sit alongside fructans in the “O” of the FODMAP acronym (Fermentable Oligo-, Di-, Mono-saccharides And Polyols). GOS are short sugar chains, usually three or four units long, held together by alpha-1,6-glycosidic bonds between galactose and glucose units. The most common members of the family in legumes are raffinose, stachyose and verbascose.
Here’s the core fact most blog articles skip. The human small intestine doesn’t produce alpha-galactosidase, the enzyme that breaks alpha-1,6 bonds. We literally can’t digest these sugars. They travel intact through your stomach and small intestine and arrive in the large colon completely unbroken.
That is where your gut bacteria find them.
The colonic flora, particularly Bifidobacterium and Faecalibacterium species, ferment GOS for energy. Fermentation produces hydrogen, carbon dioxide and, in roughly a third of people whose gut harbours Methanobrevibacter smithii, methane gas as well. A Monash University FODMAP team study found that adding GOS to a diet otherwise low in FODMAPs induced symptoms in about two-thirds of IBS participants tested. That isn’t a defect in those people. It’s a normal biological reaction to a fermentable substrate, amplified by gut sensitivity.
The whole bloating-after-dal experience is therefore not a “weak digestion” story. It’s a “your colon is doing exactly what it should, but the gas-producing load is too high for your particular nervous system to handle quietly” story.
Why Your Dadi’s Dal Didn’t Bloat You

Here’s where I think the real twist sits, and where you’ll find the practical fix. Traditional Indian cooking, when done the way our grandmothers did it, includes at least four steps that specifically reduce the GOS load before the food reaches your colon. Modern shortcuts have quietly dropped all four.
Soaking, done properly, not for fifteen minutes. Long-soaking lentils in warm water reduces phytic acid by 30 to 50 percent and dissolves a meaningful share of the GOS out of the seed and into the water. A 2018 paper in the International Journal of Food Sciences and Nutrition on five Mediterranean legumes showed that soaking and discarding the water reduced alpha-galacto-oligosaccharide content significantly across all five. Another peer-reviewed analysis found that lentils soaked at 45°C and pH 4.0 for three hours can lose up to 85 percent of their oligosaccharide content. The catch in all of these studies is the same. The dissolved GOS ends up in the soak water. Modern kitchens often dump lentils into a pressure cooker straight from the packet, or “soak for ten minutes while I chop the onions,” or (the worst version) soak the dal and then cook it in the same water. Each of these keeps the bloat-causing compounds in the bowl.
The fix: red and yellow dals like masoor and moong can get away with a 30-minute soak. Chana, rajma and whole moong need at least eight hours. The soaking water always gets discarded. Always. Then the dal is cooked in fresh water.
Hing (asafoetida), not just for flavour. Indian cooks have been adding a pinch of hing to the tadka of every dal for centuries. They had no idea about FODMAPs, but they were doing exactly the right thing. Asafoetida has measurable carminative and antispasmodic effects, including documented reductions in intestinal gas volume in animal models. Compounds in hing also stimulate pancreatic lipase secretion and the gastric phase of digestion, which means food moves faster through the upper GI tract and spends less time fermenting. Even a quarter teaspoon in the tempering meaningfully changes how a chana dal sits in your stomach.
Ajwain and jeera. Carom seeds (ajwain) are rich in thymol, which stimulates the secretion of gastric digestive enzymes and reduces intestinal gas pressure. Jeera (cumin) has well-documented carminative properties confirmed in small clinical trials in functional dyspepsia. The standard north Indian tempering (ghee, jeera, hing, sometimes ajwain) is, accidentally or otherwise, a serious digestive aid. If you do nothing else, never make a dal without these three.
You know that feeling when a dal cooked at a friend’s house sits beautifully and the same dal cooked at home leaves you uncomfortable for hours? Most of the time, it’s the tadka.
Long, slow cooking. Pressure cookers are efficient but they finish their job before the GOS chains have fully diffused out of the legume. A traditional dal (pressure-cooked first, then simmered for 30 to 45 minutes more on a low flame with the tadka and water) breaks down more of the indigestible carbohydrate. I might be wrong about how universally this applies, but in my own observation, if you eat rajma or chole regularly and bloat, this single change often helps within a week.
The Indian Context You Won’t Read Anywhere Else

A widely cited 2020 systematic review and meta-analysis in The Lancet Gastroenterology and Hepatology reported IBS prevalence in India at around 0.2 percent using strict Rome IV criteria. Startlingly low compared to neighbouring Bangladesh at 4.6 percent. The figure is almost certainly an underestimate because Rome IV is restrictive and Indian patients rarely present formally for functional gut symptoms. A college-student study from a north Indian medical college published in Neurogastroenterology and Motility in 2021 found IBS prevalence of 6.2 percent and functional dyspepsia of 15.2 percent in the same population, with non-vegetarian diet, junk food consumption, anxiety and insomnia as independent predictors.
In the real-world Indian outpatient setting, the picture an experienced gastroenterologist sees is different from the epidemiology papers. A large share of patients walking in with “gas trouble” actually have functional bloating without meeting full IBS criteria, often with overlapping post-prandial distress. They get prescribed a domperidone-PPI combination, an antispasmodic like drotaverine and sometimes a probiotic, and they come back six months later with the same complaint.
The interesting Indian-specific layer underneath this is the very high carbohydrate content of the traditional plate. A typical North Indian thali at lunch (dal, rice, two rotis, a bowl of curd, a sabzi cooked in onion-tomato gravy, a small portion of raita and pickle) contains an enormous mixed FODMAP load: GOS from the dal, fructans from the wheat and onion-garlic in the gravy, lactose from the curd, and excess fructose if a sweet follows. The bloating gets blamed on the dal because the dal is the most “suspicious” item. The real culprit is often the combined load.
This is also why low-FODMAP elimination diets, which became a major IBS management tool internationally over the last decade, struggle in India. A truly low-FODMAP Indian diet excludes onion, garlic, wheat, rajma, chole, chana, masoor in larger quantities, raita and most pickles. That eliminates roughly half of a standard kitchen. Most Indian dietitians who run low-FODMAP elimination trials report poor adherence by week three.
Diagnostic Workup — Order of Tests
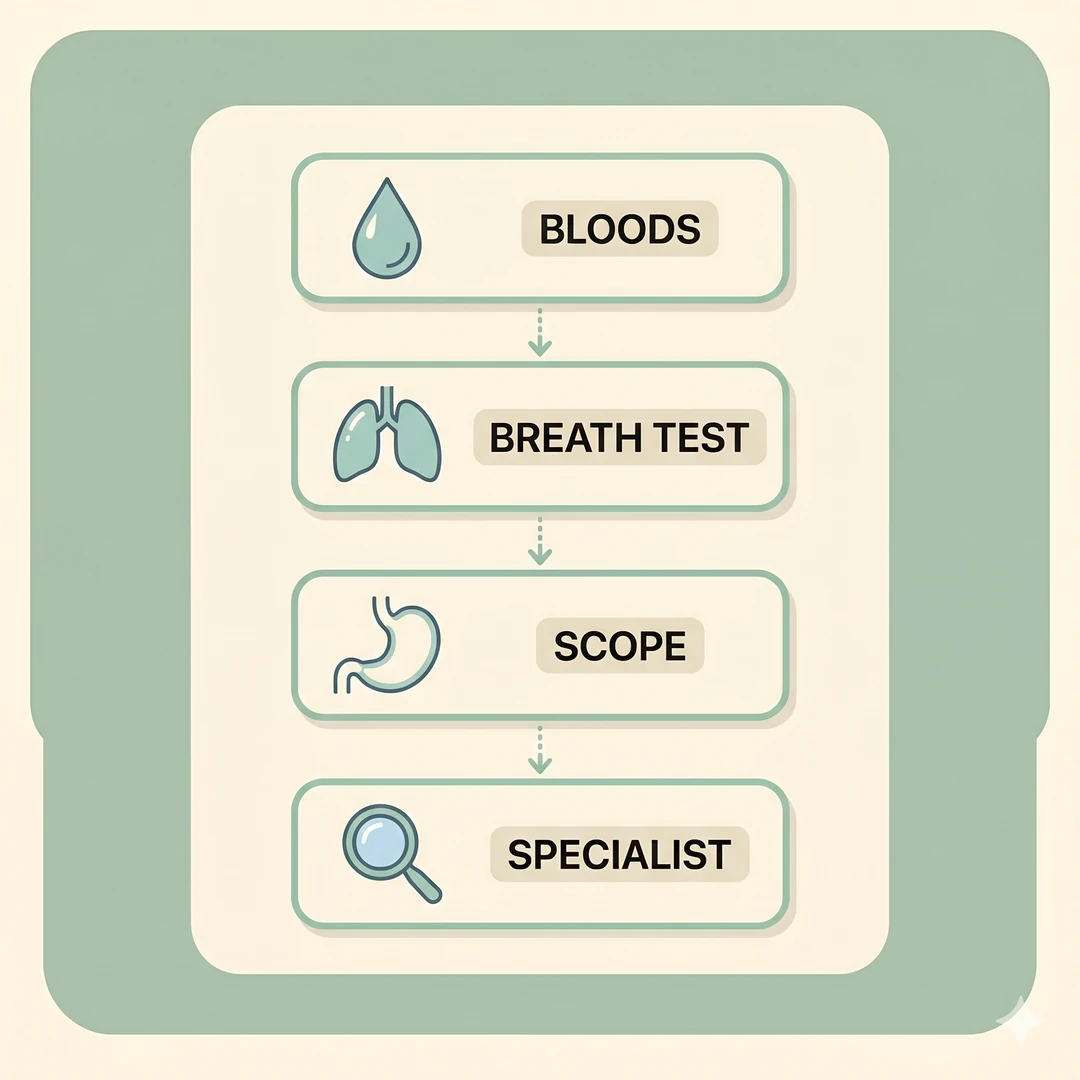
Before assuming you have functional bloating or IBS, work through the differentials. Most Indian gastroenterologists who do this carefully will go in roughly this order, and you can ask your doctor to follow it.
First visit — basic bloods and stool. Complete blood count, ferritin, vitamin B12, thyroid function (TSH, T3, T4), HbA1c, fasting glucose, liver function and stool routine with occult blood. The point of this panel isn’t to diagnose bloating. It’s to rule out hidden anaemia, hypothyroid-related constipation, undiagnosed diabetes causing motility changes, and silent GI bleeding.
Second visit — celiac and lactose. Tissue transglutaminase IgA antibody with total IgA, and a lactose hydrogen breath test. Celiac disease in India is much commoner than the textbooks suggest, particularly in north Indian wheat-eating populations, with prevalence around 0.5 to 1 percent. Lactose intolerance affects a majority of South Asian adults to some degree; a recent paper in the PMC archive on Indian IBS patients found lactose intolerance prevalence around 47 percent in IBS-D subgroup.
Third visit if symptoms continue — SIBO breath test and Rome IV checklist. Small intestinal bacterial overgrowth is increasingly diagnosed in India after the Indian Neurogastroenterology and Motility Association published the Asian-Pacific consensus in 2022. Glucose or lactulose hydrogen-methane breath testing is the standard. If positive, the standard treatment is rifaximin 550 mg three times daily for 14 days for hydrogen-dominant SIBO, or rifaximin combined with neomycin 500 mg twice daily for methane-dominant SIBO. A small Indian RCT published in the Indian Journal of Gastroenterology showed reduction of breath methane with rifaximin shortened colonic transit time and improved constipation symptoms. Cost in India runs ₹1800 to ₹2500 for a 14-day course of branded rifaximin.
Fourth visit if nothing fits — gastroenterology referral. Endoscopy with biopsies, colonoscopy if you are over 40, MRI enterography if you have suspected Crohn’s. These aren’t first-line for routine post-dal bloating, but they belong in the workup if there are red flags.
Treatment Ladder — From Free To Prescription

Step 1 — Kitchen fixes (free). Soak dal overnight in fresh water, discard the soak water, cook in fresh water. Add hing, jeera and ajwain to the tadka every single time. Pressure cook then simmer rather than just pressure cook. Eat your heavier legumes (rajma, chole, whole urad) at lunch, never at dinner. Walk for ten to fifteen minutes after meals. This single change has the strongest evidence base for reducing post-prandial bloating in functional gut disorders.
Step 2 — Meal restructuring (also free). Stop combining the heaviest fermentable load in one sitting. A dal-chawal-curd-papad-pickle thali is a stress test on your colon. Keep one or two heavy items; lose the others. Eat dinner before 8 PM. Gut motility slows significantly after sunset, and the same dal that sits fine at 1 PM can sit like a brick at 10 PM.
Step 3 — Targeted supplements (low cost). An over-the-counter alpha-galactosidase enzyme taken five minutes before a high-legume meal genuinely helps. The classic 1994 Digestive Diseases and Sciences double-blind crossover study showed it significantly reduced flatulence and bloating after a high-oligosaccharide meal compared to placebo. A 2020 pilot RCT in Neurogastroenterology and Motility on IBS patients confirmed acute symptom reduction during a GOS challenge. A 2013 paediatric RCT (Di Stefano et al.) demonstrated efficacy and safety in children with gas-related symptoms. Indian-made versions are sold under several brand names with the active ingredient typically derived from Aspergillus niger.
A probiotic strain such as Bifidobacterium lactis HN019 or Lactobacillus plantarum 299v, taken consistently for eight weeks, has modest but real evidence for reducing bloating and improving transit. Quality matters here. Cheap probiotics with overstated CFU counts on the label do nothing. Sourcing from a clinical-grade manufacturer is worth the extra hundred rupees.
Peppermint oil enteric-coated capsules (180 to 225 mg, two to three times daily before meals) have a strong evidence base in IBS-related bloating, with a 2019 meta-analysis in BMC Complementary Medicine and Therapies showing significant symptom reduction. They’re particularly useful for the painful, spasmodic component of bloating.
Step 4 — Prescription antispasmodics. Mebeverine 135 mg three times daily, or hyoscine butylbromide (Buscopan) 10 mg as needed, taken half an hour before meals. These relax smooth muscle and reduce the painful component of bloating without affecting motility much. Drotaverine (Spasmoproxyvon, Drotin) is the most prescribed antispasmodic in India but is weaker on functional bloating; mebeverine is the more rational choice.
Step 5 — Low-FODMAP elimination with a dietitian. This is a structured six-to-eight week elimination phase followed by systematic reintroduction. It works in 50 to 70 percent of people with IBS-related bloating but requires a trained dietitian to avoid nutritional deficiencies and to do the reintroduction correctly. Doing low-FODMAP from a YouTube video and staying on it forever is a common mistake that creates new problems.
Step 6 — Rifaximin if SIBO is positive. As above. Don’t take this empirically without breath test confirmation; it costs ₹1800+ and the resistance pattern is worsening with overuse.
When To Stop Self-Managing And See A Doctor

Some bloating patterns aren’t “your cooking method.” They’re red flags that demand a gastroenterologist now, not next month.
Bloating with unintentional weight loss. Blood in stool or persistent change in bowel habit. Bloating that started suddenly after age 40 without dietary change. Iron-deficiency anaemia alongside the bloating. Severe, sharp pain rather than discomfort. A family history of colon cancer or inflammatory bowel disease. Night-time waking due to gut symptoms.
These can mean celiac disease, Crohn’s, ulcerative colitis, ovarian cancer (which presents as persistent bloating in women, particularly after 50, and is consistently missed), pancreatic insufficiency, or colorectal cancer. None of them are diagnosed by guessing. Get an appointment, push for the workup, don’t let yourself be brushed off with “it’s just gas.”
What Indians Actually Say On Forums
Trawl through r/india, r/IndianFood and r/IBS, plus Quora India threads on bloating, and the genuine first-person fixes that come up again and again are not supplements.
“Soaked rajma for 12 hours, threw out the water, cooked fresh. Bloating gone.”
“Stopped eating chana at dinner. Only at lunch. Massive difference.”
“Added a pinch of hing to every dal. Don’t know why, it just works.”
“Walked for 15 minutes after lunch instead of lying down. This single thing.”
“Stopped scrolling while eating. Chewed properly. The bloating got better.”
“Pressure cooker to instant pot meant my dal was cooking in 8 minutes instead of 40. Switched back to my Hawkins. Bloating gone in two weeks.”
The science matches the lived experience exactly. The dal isn’t the problem. The way most urban Indians cook and eat it now is. I’ll admit I used to think the supplement-and-probiotic route was a reasonable first attempt before the kitchen audit; the more cases I’ve seen, the more I think that’s the wrong order.

Also Read
How to Reduce Triglycerides Without Medicine in One Month — for the lipid side of metabolic gut load.
Blood Sugar Balance at Social Events — for managing rich Indian meals at weddings without the post-meal crash.
For pharmacy-grade alpha-galactosidase, clinical-strength probiotic strains, peppermint oil enteric-coated capsules and gut-support formulations, see the full IndiaPharmaFranchise product range. Pharma entrepreneurs interested in adding well-formulated digestive products to a regional portfolio can explore the franchise opportunity.
Disclaimer: This article is general information for adult Indian readers and doesn’t replace a consultation with a gastroenterologist. Persistent bloating, especially with red flags such as weight loss, bleeding, or new onset after 40, requires medical evaluation. Don’t start or stop prescribed therapy based on a blog article.
Sources
1. Monash University FODMAP team — Including legumes on a low FODMAP diet and Cooking legumes on a low FODMAP diet. https://www.monashfodmap.com/blog/including-legumes-on-low-fodmap-diet/ and https://www.monashfodmap.com/blog/cooking-legumes/ 2. Monash University — Enzyme therapy in IBS patients sensitive to GOS. https://www.monashfodmap.com/blog/new-research-enzyme-therapy-can-help-reduce-symptoms-ibs-patients-sensitive-galacto-oligosaccharides-gos-present-legumes-soy-milk-and-nuts/ 3. Sperber AD et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021. https://www.gastrojournal.org/article/S0016-5085(20)30487-X/pdf 4. Sharma A et al. Prevalence, overlap, and risk factors for Rome IV functional gastrointestinal disorders among college students in northern India. Indian Journal of Gastroenterology 2021 (PubMed 33226570). https://pubmed.ncbi.nlm.nih.gov/33226570/ 5. Sharara AI et al. A randomized double-blind placebo-controlled crossover pilot study: Acute effects of the enzyme α-galactosidase on gastrointestinal symptoms in irritable bowel syndrome patients. Neurogastroenterology and Motility 2020 (PubMed 33619835). https://pubmed.ncbi.nlm.nih.gov/33619835/ 6. Ganiats TG et al. Does Beano prevent gas? A double-blind crossover study of oral α-galactosidase to treat dietary oligosaccharide intolerance. Digestive Diseases and Sciences 1994 (PubMed 7964541). https://pubmed.ncbi.nlm.nih.gov/7964541/ 7. Di Stefano M et al. Efficacy and tolerability of α-galactosidase in treating gas-related symptoms in children: a randomized, double-blind, placebo controlled trial. BMC Gastroenterology 2007. https://pmc.ncbi.nlm.nih.gov/articles/PMC3849317/ 8. Aguilera Y, Diaz MF et al. Oligosaccharide Content and Composition of Legumes and Their Reduction by Soaking, Cooking, Ultrasound, and High Hydrostatic Pressure. Journal of Agricultural and Food Chemistry 2009. https://www.researchgate.net/publication/228696683 9. Soaking and cooking modify the alpha-galacto-oligosaccharide and dietary fibre content in five Mediterranean legumes. International Journal of Food Sciences and Nutrition 2018. https://www.tandfonline.com/doi/full/10.1080/09637486.2018.1544229 10. Lactose Intolerance in Irritable Bowel Syndrome: Prevalence, Subtype Correlations, and Clinical Predictors in an Indian Cohort. PMC 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12740768/ 11. Ghoshal UC et al. Asian-Pacific consensus on small intestinal bacterial overgrowth in gastrointestinal disorders: An initiative of the Indian Neurogastroenterology and Motility Association. Indian Journal of Gastroenterology 2022. https://link.springer.com/article/10.1007/s12664-022-01292-x
You might also like

How to Legally Get Monobenzone Cream in Saudi Arabia, UAE, GCC, Iraq & Yemen (2026 Guide)
Country-by-country guide to legally obtaining prescription monobenzone in the GCC — SFDA, MOHAP and Oman MOH rules explained.
Read article →
كريم مونوبنزون: الدليل الشامل لعلاج البهاق المنتشر
ما هو المونوبنزون، كيف يعمل، لمن يصلح، وكيف تحصل عليه بوصفة طبية في الخليج.
Read article →
شراء كريم مونوبنزون في السعودية والخليج — الدليل العملي ٢٠٢٦
كيف تطلب مونوبنزون أصلياً بوصفة طبية إلى السعودية والإمارات وعمان — أسعار المصنع مباشرة.
Read article →